Pain is something that I see everyday! I feel as though I know it well as I have personally felt the physical components of it for much of my adult life and see it in almost every one of my patients. I have explained it while teaching around the world, developed educational curriculum around it, and here I am talking about it to you.
So, what is pain?
"Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage."
— International Association for the Study of Pain
But, what does this really mean? Well, lets look at pain and the different types of pain to determine what it means to you…
Pain is actually a good thing. It is our body's alarm system, warning us of potential or actual damage. It is designed to make us stop whatever activity might be causing the pain, so that we can investigate and correct the problem. Ignore pain, overly protecting a body part or thinking it will go away may be the worst things you do for your injury and health.
Pain is the common component to all neuro-musculo-skeletal (NMSK) conditions that result in movement dysfunction and disease. Essentially pain is the primary reason why someone goes to their family doctor, emergency room, and sees someone like myself. People looking for solutions to get them out of pain is the reason why people seek out professionals like myself.
When an injury initially occurs there is trauma to tissue and this leads to a rupture in the cell membrane (layer that encapsulates and protects) resulting in the release of fluid and chemicals into the surrounding environment. Inflammation begins when these damaged cells release various chemicals (potassium, bradykinin, and histamine, substance P, and prostaglandin E2). These chemicals are capable of activating free nerve cells in the body which tell your brain that something is wrong (nociceptive pain generators). This is called a neuro-chemical reaction. The neuro-chemical interaction initially causes muscles to be inhibited or turned off then it causes an increased neuro-muscular tone (tightening or spasm) of the muscles. This protective mechanism is used to immobilize an injured area as is initially a very good thing. However, complications arise when prolonged pain leads to inefficient movements and these lead to an increased likelihood of further tissue damage.
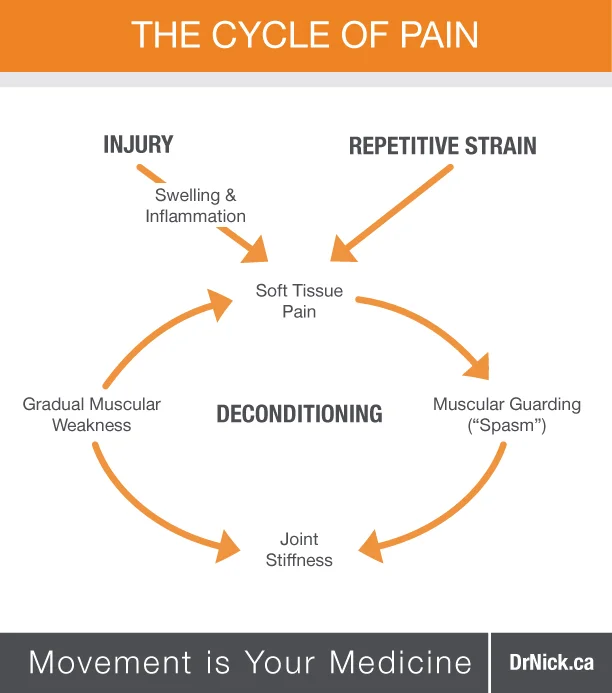
These inefficiencies in movement lead to compensations and substitution patterns which increases the mechanical stress and loads experienced by the muscles and joints involved. The body does not have an infinite amount of adaptive capabilities and sometimes something that seemed trivial ends up debilitating a patient. Ever wonder why someone says, “I didn't do anything to hurt myself, I just bent over to pick up a pencil and I was unable to get up and have been extreme pain ever since.” Well this scenario is quite normal for people with chronic dysfunction (see The Pain Cycle Diagram below). This is why my approach looks at the whole body in order to identify not only what is hurting or is in pain, but more importantly what the primary cause of the condition is/was. Once the WHY is addressed, then the HOW we are going to get you better is initiated. I say we, because your road to reaching optimal health is a process that needs both a doctor (that is me) and a patient (you) that are willing to work together and reach not only an understanding but also an active participation in doing what YOU need to do to achieve optimal health for YOU.
Now, back to the topic of pain. Well, pain is generally categorized as being either acute (as discussed previously with a trauma resulting in tissue disruption) or chronic (to be discussed more below), and may originate in skin, muscles, bones, or directly from nerves. However, pain does not always serve as a good early-warning system of something wrong as discussed previously; it often arises only after damage is done. Once damage occurs, such as a traumatic injury or repetitive strain, several biochemical processes ensue. Inflammation creates a local, followed by a global response in your body, which is assisted by pain pathways that travel from the affected part of the body to the spinal cord and end in the brain. Various chemical and neurological interactions occur that cause you to experience a certain event as painful. Traumatic injuries and repetitive stress overloads tissues and leads to their disruption and even failure. Tissue includes muscles, tendons, ligaments, bones and other forms of connective tissue, which is better known as fascia.
The perception of pain involves sensitivity to chemical changes in tissues and the interpretation that these changes are harmful. This perception is real, whether or not harm has occurred or is occurring. The brain is involved in the perception of pain. So, PAIN IS ALL IN YOUR HEAD, well, not exactly…
Pain is a mental process of what people feel after a trauma has occurred, whereas a thing called nociception is the sensory mechanism letting your spinal cord and brain know that actual trauma has occurred.
Various Types of Pain
Nociceptive pain
This is acute pain in its purest form; it tends to be localized; creates predictable responses to stretch, compression or movement (like “ouch that hurts please do not move”); often responds to simple analgesic and anti-inflammatory medication (NSAIDs), but the response is symptom based and doesn’t address the cause, in actuality it has recently been shown that using NSAIDs prevents proper tissue healing; best managed with appropriate manual therapy treatments.
Peripheral neurogenic pain
This is something I do not wish for many people to experience, there is definitely some anatomically abnormal here, and can be seen with things like Disc Injuries, and Severe Degenerative Changes; seen with acute and chronic pain; is anatomical distribution; has a burning, sharp, shooting, electrical characteristic; people often have allodynia (pain that due to a stimulus which does not normally provoke pain), dysaesthesia (unpleasant and abnormal sense of touch), parasthesia (sensation of tingling, tickling, prickling, pricking, or burning of skin with no apparent long-term physical effect) associated with it; it is provoked by nerve stretch, compression, or palpation; possibly associated muscle weakness and autonomic changes; poor response to simple analgesic and anti-inflammatory medication, often requires stronger medications if necessary; response to manual therapy treatment varies, a more subtle treatment modality is best; laser and acupuncture helps; diet modification and creating an anti-inflammatory environment in the body is beneficial.
Central sensitization
This is one of the processes in which acute pain becomes chronic pain; it is often widespread, and has a non-anatomical distribution, i.e., it is all over the place; Hyperalgesia (increased sensitivity to pain) and allodynia are often associated with this; Inconsistent response to stimuli and test; pharmaceutical treatment is primarily ineffective
There are certain features that are commonly involved in causing or intensifying pain. It is important to understand their existence so that when they present themselves you can attempt to avoid them and address them appropriately. The following factors either affect the body as a whole or as individual parts.
Factors That Can Affect the Whole Body's Perception of Pain
- Genetic predisposition, e.g., connective tissue factor leading to hypermobility, and inborn anomalies, e.g., short leg
- Nutritional imbalances and deficiencies
- Toxicity (exogenous and endogenous)
- Infections (chronic and acute)
- Endocrine imbalances
- Stress (physical and psychological)
- Trauma
- Posture (including patterns of misuse)
- Hyperventilation tendencies
Factors That Can Affect Local Areas of Pain or Discomfort
- Hypertonia (tight muscles)
- Ischemia (lack of blood flow)
- Inflammation
- Trigger points
- Neural compression or entrapment
Current research has now shown that acute pain and chronic pain are distinct entities physiologically, neuroanatomically, and psychologically. Chronic pain is not just acute pain that occurs over a long period of time, which is what was believed for many years, but rather a disease that has developed through biochemical and anatomical changes in the nervous system.
Transition From Acute to Chronic Pain
There are various factors that play a role in the presentation of acute pain and the development of chronic pain. These are biomechanical (congenital, overuse, misuse, trauma); biochemical (toxins, hormonal problems, nutritional deficiency, lack of oxygen, inflammation); and psychosocial (anxiety, depression, unresolved emotional states). In order to appropriately treat the various factors associated with acute and chronic pain, many different but interrelated approaches must be used. To effectively influence the biomechanical factors, physical medicine [hyperlink] and active rehabilitation [hyperlink] should be utilized. To deal with biochemical influences, nutritional or pharmaceutical tactics are used. Lastly, to appropriately deal with psychosocial influences various psychological approaches are used. To find the most appropriate person to manage the biochemical and psychological factors I refer to a variety of allied health care professionals that I feel will work well with your personality and needs. Ask me for more details.
Persistent or chronic pain is associated with what is called neuroplastic changes. Neuroplasticity is characterized by the ability of our nervous system to adapt and change in response to the demands placed on it. These adaptations of the nervous occur at various levels within the spinal cord and brain (it actually occurs at primary afferent neurons, the spinal cord, brainstem, thalamus, limbic system and cortex, if you want to be exact). And with these changes, if there are other factors stressing and creating further inputs to these brain centers there is more neuroplasticity occurring. The adaptations that ensue often result in disproportionate responses to what is thought of as innocuous stimuli causing extreme pain. It is important to understand that plasticity indicates just that, the ability for something to change over time and the potential for reversibility and Chronic Pain is not a life sentence. There are solutions and the methods of managing both acute and chronic pain can sometimes be much simpler than many think. But what seems simple is not always easy.
So, when a patient begins to experience persistent pain, the pain pathways and processing centers become conditioned to maintain their post-injury activity long after the insulting trauma has passed and the tissue has, for all intensive purposes, healed. This persistence effectively changes the way you perceive the pain and since neuroplasticity is dependent on input, the lack of movement after a fall, resting an injury or “babying” a body part can essentially push you towards feeling pain, rather than feeling as though you can move. This in addition to the increased muscle tone and inhibition of affected muscles and surrounding muscles leads to further problems. Therefore, not moving could be the single worst thing you can possibly do for yourself after you have hurt a body part. Now the fear of moving is real, not many people like to feel pain so they avoid movement at all costs, unless they are under the care of someone skillful who know what to do and how to do it so that the tissue is protected and you are on your way to recovery. Therefore, it is important that an injured area be continuously moved in a safe and effective manner, not forcing the healing structures to experience a load it cannot handle, but rather be put through motions that develop tensile strength while at the same time ensuring that your muscles and brain do not deteriorate and perpetuate chronic pain behaviour. Hence, why movement is YOUR medicine. But with all Medicine there are precautions. If you have any questions about how to manage your condition, visit the ever-developing library of conditions on this site, or Ask Me a question and I would be happy to help.
Adaptation to Tissue Disruption and Deconditioning
Deconditioning not only affects the structure of muscles and joints, but also the information that enters the spinal cord and brain from receptors within muscles, joints ligaments and skin which allows the brain to know where each part of your body is in space (proprioception). This proprioception allows for your body to maintain balance, posture and co-ordinate movements. People in pain typically become inactive and this can contribute to deconditioning. With deconditioning the body can be more susceptible to postural or occupational repetitive strains. A chronic cycle of recurring pain is easily established unless proper function is restored. Treatment for pain relief alone will not reverse the deconditioning and various functional problems. Proper management is not based on just relieving pain but also promoting healing and restoring proper body function to prevent recurrence.
The Pain Cycle often shows how deconditioning occurs
The best treatment is often prevention.
You must have heard the old saying that an ounce of prevention is worth a pound of cure. Well, the more external stress, the greater the chance of injury. External stressors can include prolonged sitting, improper lifting technique, or repetitive activities. Internal factors such as imbalances of muscle strength or flexibility, poor posture, structural problems (i.e., short leg), impaired coordination or balance, or poor cardiovascular fitness also predispose to recurrent pain episodes. And when treatment is required, it all depends when in the healing process it is started and what the best mode of care for the specific individual experiencing their symptoms and/or condition.
Tissue Trauma and the Phases of Healing/Treatment
Acute Phase
This lasts 24 to 72 hours after an injury. This is when inflammation and muscle guarding is present. The goal of treatment here is to manage swelling and pain. This is accomplished with the aid of nutraceuticals (vitamins, minerals, herbals and homeopathic remedies) and/or pharmaceuticals (non-steroidal anti-inflammatory (NSAIDs) or some pain medication. As I am not licensed to provide pharmaceutical information, I relinquish that advice to be provided by a medical physician or pharmacist. But, when talking about Non-pharmacological methods to reduce inflammation and swelling include, well this I know a thing or two about. You can use ice, electrotherapies (such as laser and frequency specific microcurrent), acupuncture and nutraceuticals. I always recommend relative immobilization with the use of kinesiology tape, ice and traumeel as the best first aid treatment for the first 72 hours after an injury and will discuss more about icing and first aid care in another article.
Sub-acute Phase
This lasts from 24 hours to 6 weeks. This is when tissue repair and regeneration occurs. During this time it is important that a patient with a sub-acute injury understands that their tissues are going through repair and that healing needs to occur. Violent activities that exceed the bodies ability to adapt needs to be prevented. Faulty movement patterns and weakened muscles and tissues need to be addressed. This is done through the use of various passive treatment methods, what I call physical medicine such as kinesiology taping, joint manipulation or mobilization, soft tissue therapies, electrotherapies and acupuncture to normalize tissue mobility and blood supply as well as engaging in the appropriate active rehabilitation exercises to developing proper strength, stability, endurance and coordination of movements so that the healing tissues and the compensatory tissue that were not working well start properly develop and you prevent deconditioning from occurring.
Remodeling
This starts at approximately the third week after an injury and can take up to 12 months to be complete. It is important that a patient strengthens and stabilizes their "weak link" or injured tissues to prevent recurrences. With appropriate physical medicine, and active rehabilitation you can return to or exceed your pre-injury function.
If you or someone you know has pain and would like to learn more about how to better manage it, feel free to share this or have them (or you) contact me to ask me how I may be of service to you.